Each tablet contains 80 mg of febuxostat.
Excipients/Inactive Ingredients: Tablet core: Microcrystalline Cellulose 101; Microcrystalline Cellulose 102; Lactose Monohydrate; Croscarmellose Sodium; Hydroxypropylcellulose; Colloidal Anhydrous Silica; Magnesium stearate.
Tablet coating: Opadry II 85F42129 Yellow containing: Polyvinyl Alcohol Part. Hydrolyzed; Titanium Dioxide (E171); Macrogol/PEG; Talc; Iron Oxide Yellow (E172).
Treatment of chronic hyperuricaemia in conditions where urate deposition has already occurred (including a history, or presence of, tophus and/or gouty arthritis).
Febuxostate Pentafarma Tablets 80mg is indicated in adults.
Posology: The recommended oral dose of Febuxostate Pentafarma Tablets 80mg is 80 mg once daily without regard to food. If serum uric acid is >6 mg/dL (357 μmol/L) after 2-4 weeks, febuxostat 120 mg once daily may be considered.
Febuxostate Pentafarma Tablets 80mg works sufficiently quickly to allow retesting of the serum uric acid after 2 weeks. The therapeutic target is to decrease and maintain serum uric acid below 6 mg/dL (357 μmol/L).
Gout flare prophylaxis of at least 6 months is recommended.
[Note: 120 mg tablet is currently not available in this product. This product is not sub-dividable. Physicians should consider using other brands in the market for 120mg.]
Elderly: No dose adjustment is required in the elderly.
Renal impairment: The efficacy and safety have not been fully evaluated in patients with severe renal impairment (creatinine clearance <30 mL/min).
No dose adjustment is necessary in patients with mild or moderate renal impairment.
Hepatic impairment: The efficacy and safety of febuxostat has not been studied in patients with severe hepatic impairment (Child Pugh Class C).
The recommended dose in patients with mild hepatic impairment is 80 mg. Limited information is available in patients with moderate hepatic impairment.
Pediatric population: The safety and the efficacy of febuxostat in children aged below the age of 18 years have not been established. No data are available.
Method of administration: Oral use.
Febuxostate Pentafarma Tablets 80mg should be taken by mouth and can be taken with or without food.
Patients with an overdose should be managed by symptomatic and supportive care.
Hypersensitivity to the active substance or to any of the excipients.
Cardio-vascular disorders: Treatment with febuxostat in patients with pre-existing major cardiovascular diseases (e.g. myocardial infarction, stroke or unstable angina) should be avoided, unless no other therapy options are appropriate.
A numerical greater incidence of investigator-reported cardiovascular APTC events (defined endpoints from the Anti-Platelet Trialists' Collaboration (APTC) including cardiovascular death, non-fatal myocardial infarction, non-fatal stroke) was observed in the febuxostat total group compared to the allopurinol group in the APEX and FACT studies (1.3 vs. 0.3 events per 100 Patient Years (PYs)), but not in the CONFIRMS study. The incidence of investigator-reported cardiovascular APTC events in the combined Phase 3 studies (APEX, FACT and CONFIRMS studies) was 0.7 vs. 0.6 events per 100 PYs. In the long-term extension studies the incidences of investigator-reported APTC events were 1.2 and 0.6 events per 100 PYs for febuxostat and allopurinol, respectively. No statistically significant differences were found and no causal relationship with febuxostat was established. Identified risk factors among these patients were a medical history of atherosclerotic disease and/or myocardial infarction, or of congestive heart failure.
In the post registrational CARES trial the rate of MACE events was similar in febuxostat versus allopurinol treated patients (HR 1.03; 95% CI 0.87-1.23), but a higher rate of cardiovascular deaths was observed (4.3% vs. 3.2% of patients; HR 1.34; 95% CI 1.03-1.73).
Medicinal product allergy/hypersensitivity: Rare reports of serious allergic/hypersensitivity reactions, including life-threatening Stevens Johnson Syndrome, Toxic epidermal necrolysis and acute anaphylactic reaction/shock, have been collected in the post-marketing experience. In most cases, these reactions occurred during the first month of therapy with febuxostat. Some, but not all of these patients reported renal impairment and/or previous hypersensitivity to allopurinol. Severe hypersensitivity reactions, including Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS) were associated with fever, hematological, renal or hepatic involvement in some cases.
Patients should be advised of the signs and symptoms and monitored closely for symptoms of allergic/hypersensitivity reactions. Febuxostat treatment should be immediately stopped if serious allergic/hypersensitivity reactions, including Stevens-Johnson Syndrome, occur since early withdrawal is associated with a better prognosis. If patient has developed allergic/hypersensitivity reactions including Stevens-Johnson Syndrome and acute anaphylactic reaction/shock, febuxostat must not be re-started in this patient at any time.
Acute gouty attacks (gout flare): Febuxostat treatment should not be started until an acute attack of gout has completely subsided. Gout flares may occur during initiation of treatment due to changing serum uric acid levels resulting in mobilization of urate from tissue deposits. At treatment initiation with febuxostat flare prophylaxis for at least 6 months with an NSAID or colchicine is recommended.
If a gout flare occurs during febuxostat treatment, it should not be discontinued. The gout flare should be managed concurrently as appropriate for the individual patient.
Continuous treatment with febuxostat decreases frequency and intensity of gout flares.
Xanthine deposition: In patients in whom the rate of urate formation is greatly increased (e.g. malignant disease and its treatment, Lesch-Nyhan syndrome) the absolute concentration of xanthine in urine could, in rare cases, rise sufficiently to allow deposition in the urinary tract. As there has been no experience with febuxostat, its use in these populations is not recommended.
Mercaptopurine/azathioprine: Febuxostat use is not recommended in patients concomitantly treated with mercaptopurine/azathioprine as inhibition of xanthine oxidase by febuxostat may cause increased plasma concentrations of mercaptopurine/azathioprine that could result in severe toxicity. No interaction studies have been performed in humans.
Where the combination cannot be avoided, a reduction of the dose of mercaptopurine/azathioprine is recommended. Based on modelling and simulation analysis of data from a pre-clinical study in rats, when co-administered with febuxostat, the dose of mercaptopurine/azathioprine should be reduced to the 20% or less of the previously prescribed dose in order to avoid possible hematological effects.
The patients should be closely monitored and the dose of mercaptopurine/azathioprine should be subsequently adjusted based on the evaluation of the therapeutic response and the onset of eventual toxic effects.
Organ transplant recipients: As there has been no experience in organ transplant recipients, the use of febuxostat in such patients is not recommended.
Theophylline: Co-administration of febuxostat 80 mg and theophylline 400mg single dose in healthy subjects showed absence of any pharmacokinetic interaction. Febuxostat 80 mg can be used in patients concomitantly treated with theophylline without risk of increasing theophylline plasma levels. No data is available for febuxostat 120 mg.
Liver disorders: During the combined phase 3 clinical studies, mild liver function test abnormalities were observed in patients treated with febuxostat (5.0%). Liver function test is recommended prior to the initiation of therapy with febuxostat and periodically thereafter based on clinical judgment.
Thyroid disorders: Increased TSH values (>5.5 μIU/mL) were observed in patients on long-term treatment with febuxostat (5.5%) in the long term open label extension studies. Caution is required when febuxostat is used in patients with alteration of thyroid function.
Lactose: Febuxostate Pentafarma Tablets 80mg tablets contain lactose. Patients with rare hereditary problems of galactose intolerance, the Lapp lactase deficiency or glucose-galactose malabsorption should not take this medicine.
Effects on ability to drive and use machines: Somnolence, dizziness, paraesthesia and blurred vision have been reported with the use of Febuxostat. Patients should exercise caution before driving, using machinery or participating in dangerous activities until they are reasonably certain that febuxostat does not adversely affect performance.
Pregnancy: Data on a very limited number of exposed pregnancies have not indicated any adverse effects of febuxostat on pregnancy or on the health of the foetus/new born child. Animal studies do not indicate direct or indirect harmful effects with respect to pregnancy, embryonal/foetal development or parturition. The potential risk for human is unknown. Febuxostat should not be used during pregnancy.
Breastfeeding: It is unknown whether febuxostat is excreted in human breast milk. Animal studies have shown excretion of this active substance in breast milk and an impaired development of suckling pups. A risk to a suckling infant cannot be excluded. Febuxostat should not be used while breastfeeding.
Fertility: In animals, reproduction studies up to 48 mg/kg/day showed no dose-dependent adverse effects on fertility. The effect of febuxostat on human fertility is unknown.
Summary of the safety profile: The most commonly reported adverse reactions in clinical trials (4,072 subjects treated at least with a dose from 10 mg to 300 mg) and post-marketing experience are gout flares, liver function abnormalities, diarrhea, nausea, headache, rash and edema. These adverse reactions were mostly mild or moderate in severity. Rare serious hypersensitivity reactions to febuxostat, some of which were associated to systemic symptoms, and rare events of sudden cardiac death, have occurred in the post-marketing experience.
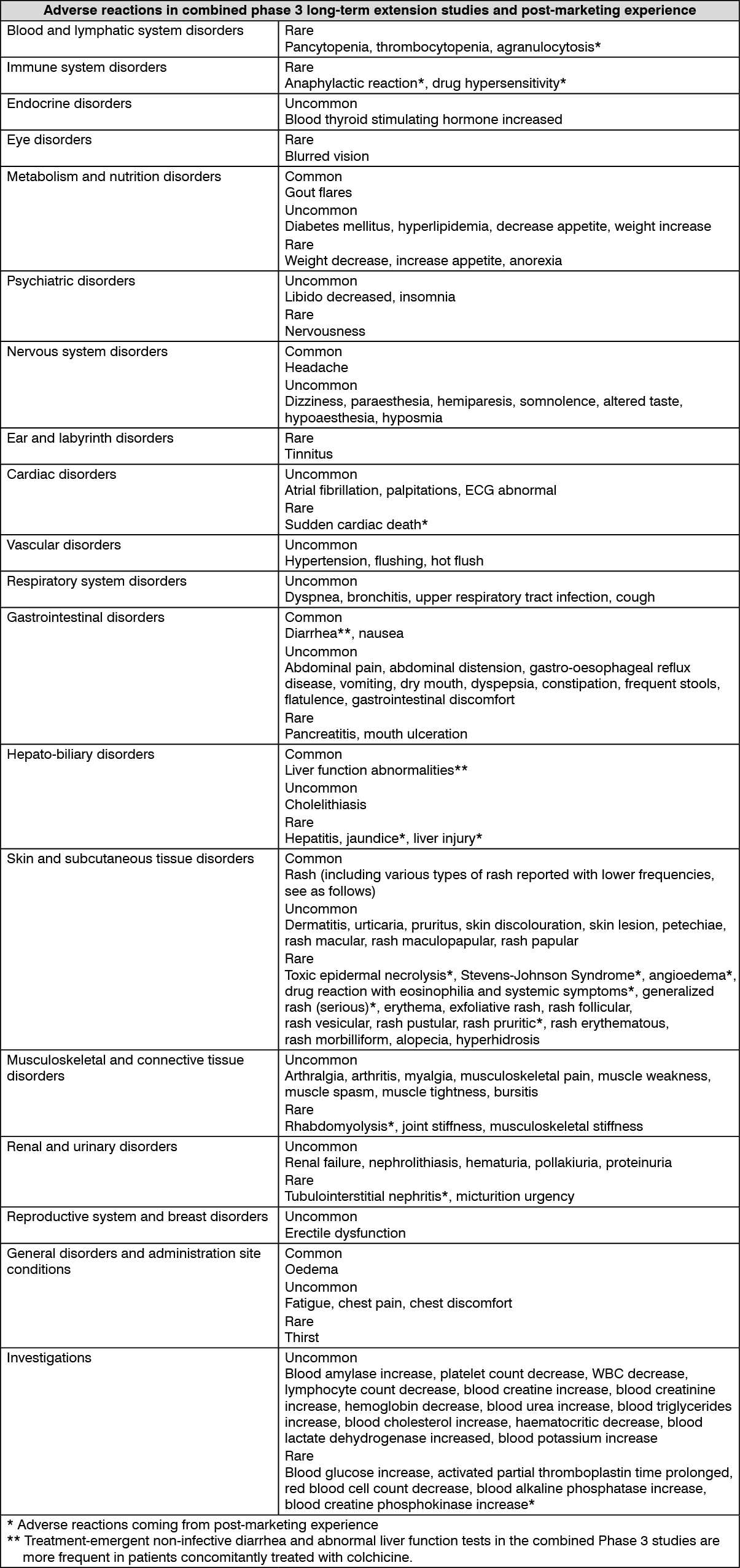
Tabulated list of adverse reactions: Common (≥1/100 to <1/10), uncommon (≥1/1,000 to <1/100) and rare (≥1/10,000 to <1/1,000) adverse reactions occurring in patients treated with febuxostat are listed as follows.
Within each frequency grouping, adverse reactions are presented in order of decreasing seriousness. (See table.)
 Click on icon to see table/diagram/image
Description of selected adverse reactions:
Click on icon to see table/diagram/image
Description of selected adverse reactions: Rare serious hypersensitivity reactions to febuxostat, including Stevens-Johnson Syndrome, Toxic epidermal necrolysis and anaphylactic reaction/shock, have occurred in the post-marketing experience. Stevens-Johnson Syndrome and Toxic epidermal necrolysis are characterized by progressive skin rashes associated with blisters or mucosal lesions and eye irritation. Hypersensitivity reactions to febuxostat can be associated to the following symptoms: skin reactions characterized by infiltrated maculopapular eruption, generalized or exfoliative rashes, but also skin lesions, facial oedema, fever, hematologic abnormalities such as thrombocytopenia and eosinophilia, and single or multiple organ involvement (liver and kidney including tubulointerstitial nephritis).
Gout flares were commonly observed soon after the start of treatment and during the first months. Thereafter, the frequency of gout flare decreases in a time-dependent manner. Gout flare prophylaxis is recommended.
Mercaptopurine/azathioprine: On the basis of the mechanism of action of febuxostat on XO inhibition concomitant use is not recommended. Inhibition of XO by febuxostat may cause increased plasma concentrations of these drugs leading to toxicity. Drug interaction studies of febuxostat with drugs (except theophylline) that are metabolized by XO have not been performed in humans.
Modelling and simulation analysis of data from a pre-clinical study in rats indicates that, in case of concomitant administration with febuxostat, the dose of mercaptopurine/azathioprine should be reduced to 20% or less of the previously prescribed dose.
Drug interaction studies of febuxostat with other cytotoxic chemotherapy have not been conducted. No data is available regarding the safety of febuxostat during other cytotoxic therapy.
Rosiglitazone/CYP2C8 substrates: Febuxostat was shown to be a weak inhibitor of CYP2C8 in vitro. In a study in healthy subjects, co-administration of 120 mg febuxostat QD with a single 4 mg oral dose of rosiglitazone had no effect on the pharmacokinetics of rosiglitazone and its metabolite N-desmethyl rosiglitazone, indicating that febuxostat is not a CYP2C8 enzyme inhibitor in vivo. Thus, co-administration of febuxostat with rosiglitazone or other CYP2C8 substrates is not expected to require any dose adjustment for those compounds.
Theophylline: An interaction study in healthy subjects has been performed with febuxostat to evaluate whether the inhibition of XO may cause an increase in the theophylline circulating levels as reported with other XO inhibitors. The results of the study showed that the co-administration of febuxostat 80 mg QD with theophylline 400 mg single dose has no effect on the pharmacokinetics or safety of theophylline. Therefore no special caution is advised when febuxostat 80 mg and theophylline are given concomitantly. No data is available for febuxostat 120 mg.
Naproxen and other inhibitors of glucuronidation: Febuxostat metabolism depends on Uridine Glucuronosyl Transferase (UGT) enzymes. Medicinal products that inhibit glucuronidation, such as NSAIDs and probenecid, could in theory affect the elimination of febuxostat. In healthy subjects concomitant use of febuxostat and naproxen 250 mg twice daily was associated with an increase in febuxostat exposure (Cmax 28%, AUC 41% and t1/2 26%). In clinical studies the use of naproxen or other NSAIDs/Cox-2 inhibitors was not related to any clinically significant increase in adverse events.
Febuxostat can be co-administered with naproxen with no dose adjustment of febuxostat or naproxen being necessary.
Inducers of glucuronidation: Potent inducers of UGT enzymes might possibly lead to increased metabolism and decreased efficacy of febuxostat. Monitoring of serum uric acid is therefore recommended 1-2 weeks after start of treatment with a potent inducer of glucuronidation. Conversely, cessation of treatment of an inducer might lead to increased plasma levels of febuxostat.
Colchicine/indometacin/hydrochlorothiazide/warfarin: Febuxostat can be co-administered with colchicine or indomethacin with no dose adjustment of febuxostat or the co-administered active substance being necessary.
No dose adjustment is necessary for febuxostat when administered with hydrochlorothiazide.
No dose adjustment is necessary for warfarin when administered with febuxostat. Administration of febuxostat (80 mg or 120 mg once daily) with warfarin had no effect on the pharmacokinetics of warfarin in healthy subjects. INR and Factor VII activity were also not affected by the co-administration of febuxostat.
Desipramine/CYP2D6 substrates: Febuxostat was shown to be a weak inhibitor of CYP2D6 in vitro. In a study in healthy subjects, 120 mg Febuxostat QD resulted in a mean 22% increase in AUC of desipramine, a CYP2D6 substrate indicating a potential weak inhibitory effect of febuxostat on the CYP2D6 enzyme in vivo.
Thus, co-administration of febuxostat with other CYP2D6 substrates is not expected to require any dose adjustment for those compounds.
Antacids: Concomitant ingestion of an antacid containing magnesium hydroxide and aluminum hydroxide has been shown to delay absorption of febuxostat (approximately 1 hour) and to cause a 32% decrease in Cmax, but no significant change in AUC was observed. Therefore, febuxostat may be taken without regard to antacid use.
M04AA03 - febuxostat ; Belongs to the class of preparations inhibiting uric acid production. Used in the treatment of gout.
Febuxostate Pentafarma FC tab 80 mg
2 × 14's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out